Trocar for Correct Chest Tube Placement
PROBLEM
From a patient point of view, a misplaced chest tube is life threatening, painful, and increases expenses. Twenty-five to 50% of tube thoracostomies result in complications (1-3). From a clinician point of view, there is excess resource use to replace improperly placed tubes. Chest tube related complications, such as recurrent pneumothorax, retained hemothorax, and empyema, frequently require additional invasive procedures ranging from the reinsertion of a new chest tube to video assisted thoracoscopic surgery or thoracotomy (4). This is also a quality concern – why place chest tubes blindly when there is a simply technology to improve this? Payers wants smarter placement to prevent complications – this problem is a target for payers to refuse payment for procedures needed in response to incorrect chest tube placement. Trocars are a type of surgical access device that can be used to access the organ or body space. However, it can be difficult for even experienced medical professionals to access organs and body spaces quickly and accurately without causing patient discomfort, without causing inadequate drainage, and/or without first experiencing one or more failed attempts in inserting the trocar into the patient. These risks are increased in obese patients and muscular patients. There remains a need for improved surgical trocar and for the development of trocars for chest tube insertions.
SOLUTION
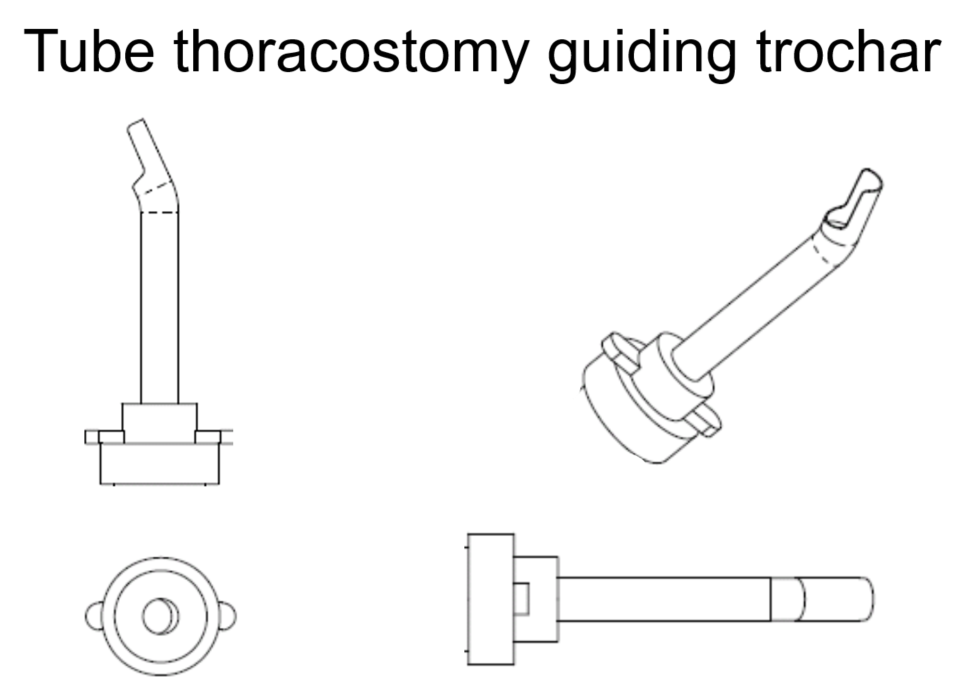
The Trocar for Correct Chest Tube Placement is an angled surgical trocar, a medical tool that will allow medical professionals to access the body cavity of a patient. The goal of the system is to avoid placing chest tubes into the lung fissure or other unwanted locations. This tool is vital to avoid the misplacement and incorrectly angled chest tube complications mentioned here. While the first indication for use of the angled trocar is the chest tube, it may be relevant for other indications as well.
This trocar fits directly into the existing workflow of chest tube placement. Utilizing a standard chest tube incision and blunt entry into the thoracic cavity allows placement of the chest tube trocar into the cavity. Once the trocar is in place the tube is inserted through the trocar and guided into the patient’s chest cavity.
VALUE/BENEFIT
The angled surgical trocar could prevent 300,000 to 790,000 complications a year. Avoiding these complications would save a tremendous amount of hospital costs and preclude patients from the difficulties that follow these complications.
References
1. Gilbert TB, McGrath BJ, Soberman M. Chest tubes: indications, placement, management and complications. J Intensive Care Med 1993; 8:73-86.
2. Tait P, Waheed U, Bell S. Successful removal of malpositioned chest drain within the liver by embolization of the transhepatic track. Cardiovasc Intervent Radiol. 2009; 32:825–7.
3. Can J Surg, Chest tube complications: how well are we training our residents? 2007. https://www.ncbi.nlm.nih.gov/pubmed/18053373
4. Osinowo O, Softah AL, Eid Zahrani M. Ectopic chest tube insertions: Diagnosis and strategies for prevention. Afr J Med Med Sci. 2002. https://www.ncbi.nlm.nih.gov/pubmed/12518934
5. Nahum E, Ben-Ari J, Schonfeld T, Horev G. Acute diaphragmatic paralysis caused by chest-tube trauma to phrenic nerve. Pediatr Radiol. 2001. https://www.ncbi.nlm.nih.gov/pubmed/11436893
Project Details
Categories:
Inventor Name: Michael Robich, MD
Inventor Name (additional): n/a
Case Number: MMC-103
Patent Application Number: PCT/US19/14881
IP Status: Filed