A Self-expanding Retrohepatic Covered Vena Caval Stent
PROBLEM
The inferior vena cava is one of the two largest veins in the body; it drains blood from the lower half of the body. The portion of the IVC that lies behind the liver is called the retro-hepatic inferior vena cava (RHIVC). The RHIVC is about 10 cm long and has 3 large tributaries (the right, middle and left hepatic veins). Of note, the right hepatic vein typically terminates within 1 cm of the diaphragm. Injury to the IVC is rare (<1% of all traumas) and accounts for 20% of abdominal vascular injuries. Owever, it carries a very fatality rate of 70 – 90%. Injury to the RHIVC and/or connected hepatic veins (See figure 1) is the second commonest type of IVC injury; “It is a trauma surgeon’s worst nightmare” as it is often fatal. Surgical access to this area is difficult because it is largely covered by the liver. These anatomical factors make for a time consuming, technically challenging mobilization that allows continuing hemorrhage, increasing coagulopathy and consequently causing fatal hemorrhage.
SOLUTION
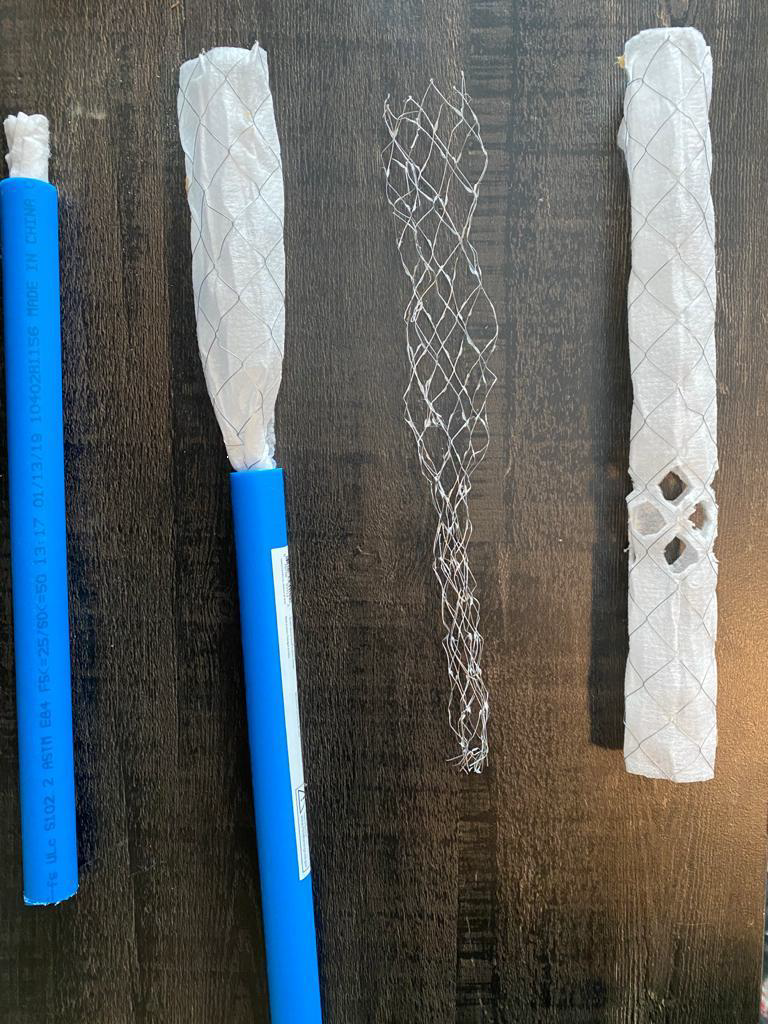
The RHIVC covered stent is a catheter-based self-expandable that is inserted into the inferior vena cava or its tributaries. The device is used to cannulate the vein or can be inserted through a venotomy below the level of the injury to the cava. Next it is advanced upwards beyond the level of the injury. The sheath of the device is withdrawn, leading to a self-deployment of the covered stent, which then occludes the hole or injury in the vein or vena cava and temporizes the bleeding from the IVC. This then allows the surgeon time to identify and repair the injury to the vena cava or its tributaries.
VALUE/BENEFIT
This device is inserted into the lower part of the IVC or it’s tributaries, and it takes advantage of the fact that a laparotomy has been performed. It does not need a thoracotomy (chest incision) thus it is less morbid that the atriocaval shunt. Further, avoids the additional risk, morbidity, and attendant complications of cutting into the patient heart. These are the advantages of my proposed device and technique over the Shrock shunt. The RHIVC covered stent can also be inserted from above the IVC through any tributaries of the superior vena cava. In this approach, it would be inserted percutaneously through a tributary of the SVC through the right atrium into the inferior vena cava to a point cephalad to the renal veins. In this approach, the RHIVC covered stent would be deployed to cover the IVC above the renal veins but below the IVC’s point of termination into the right atrium. In comparison to the total isolation of the RHIVC, this proposed technique and the RHIVC covered stent device still maintains the patency of the lumen of the vena cava, thereby preserving venous return to the heart and maintaining the preload, thus preventing the adverse cardiovascular and physiologic consequences of doubly clamping the IVC as would occur with the total IVC isolation. Therefore our approach is more physiologic and would limit the morbidity and mortality associated with total IVC isolation/clamping of the IVC.
Project Details
Categories:
Inventor Name: Obieze Nwanna-Nzewunwa, MD
Inventor Name (additional): n/a
Case Number: MMC 125
Patent Application Number:
IP Status: Provisional